AERD Risk Assessment Tool
This assessment tool helps you determine if your symptoms match Aspirin-Exacerbated Respiratory Disease (AERD), also known as Samter's Triad. AERD is a condition where asthma, chronic nasal polyps, and sensitivity to aspirin or NSAIDs occur together.
Based on research, having two or more of these symptoms increases the likelihood of AERD. This tool is not a diagnosis but can help you discuss your symptoms with a healthcare provider.
What Is Aspirin-Exacerbated Respiratory Disease?
Aspirin-Exacerbated Respiratory Disease is a chronic condition where asthma, chronic nasal polyps, and sensitivity to aspirin or NSAIDs occur together. It’s also known as Samter’s Triad or NSAID-ERD. Unlike typical allergies, this isn’t caused by an immune reaction to the drug itself. Instead, it’s a metabolic dysfunction in how your body handles inflammation.
People with AERD don’t suddenly become sensitive to aspirin. The condition develops over time, usually in adulthood between ages 20 and 50. It hits about 9% of all adults with asthma - and up to 30% of those who also have nasal polyps. The trigger isn’t the drug. It’s what happens inside your body when you take it.
How AERD Changes Your Body’s Chemistry
When you take aspirin or NSAIDs like ibuprofen or naproxen, they block an enzyme called COX-1. For most people, that’s fine - it reduces pain and swelling. But in AERD, blocking COX-1 throws your body’s inflammatory system out of balance.
Your body starts producing too much of certain inflammatory chemicals called leukotrienes, especially leukotriene E4. At the same time, it makes less of prostaglandin E2, which normally keeps inflammation in check. This imbalance turns your airways into a storm zone. Your nose swells, your sinuses get clogged, and your lungs tighten up.
Studies show this triggers a strong Type 2 immune response - think high levels of IL-4, IL-13, and IL-5. These signals pull in eosinophils, a type of white blood cell that causes tissue damage. That’s why nasal polyps grow back so fast after surgery in AERD patients.
What Happens When You Take NSAIDs?
For someone with AERD, taking even a regular dose of ibuprofen can cause a reaction within 30 to 120 minutes. Symptoms aren’t mild. They’re intense and often scary.
- Severe nasal congestion - happens in 95% of reactions
- Frontal headache or sinus pressure - 88%
- Red, watery eyes - 76%
- Wheezing, chest tightness, coughing - 92%
Some people also get nausea, vomiting, stomach pain, flushing, or a rash. These reactions aren’t random. They’re predictable. And they’re not just about the nose or lungs. The whole respiratory system goes into overdrive.
What’s surprising to many? Alcohol can trigger the same reaction in about 75% of AERD patients. You don’t need to get drunk. Even one glass of wine or beer can cause congestion, coughing, or wheezing. This isn’t about the alcohol content - it’s about how it interacts with your inflamed airways.
Why AERD Is Worse Than Regular Asthma
AERD isn’t just asthma with a side of nasal polyps. It’s a more aggressive, harder-to-control version.
People with AERD have:
- Polyps that grow back faster - 70-100% recur within 18 months after surgery
- Worse asthma control - only 35% respond well to standard inhalers
- More ER visits - 2.3 times more than non-AERD asthma patients
- More hospital stays - 1.8 times more frequent
Standard asthma treatments like albuterol or inhaled steroids often don’t cut it. That’s because the inflammation driving AERD isn’t the same kind as in allergic asthma. It’s deeper, more systemic, and harder to quiet with typical meds.
Many patients end up needing multiple sinus surgeries. But removing polyps doesn’t fix the root problem. The inflammation keeps coming back. That’s why just avoiding NSAIDs isn’t enough - it doesn’t slow the disease.
The Long Road to Diagnosis
Most people with AERD wait years before getting the right diagnosis. On average, it takes 7 to 10 years.
Why? Because doctors don’t always connect the dots. A patient might see an allergist for asthma, an ENT for polyps, and a GP for headaches - but no one puts it all together. Reddit user PolypWarrior87 shared how it took 11 years and four specialists before someone finally linked their asthma attacks to Advil and their polyps.
There’s a pattern: adult-onset asthma + recurring nasal polyps + reaction to NSAIDs or alcohol. That’s the triad. If you have two of those, you should be tested. If you have all three, it’s almost certainly AERD.
Yet, many primary care doctors and even some allergists miss the alcohol trigger. One study found that 75% of AERD patients react to alcohol - but only a fraction of clinicians ask about it.
The Only Treatment That Actually Works
There’s one treatment that changes the course of AERD: aspirin desensitization.
This isn’t a cure. But it’s the closest thing we have. In a controlled hospital setting, patients are given gradually increasing doses of aspirin over two to three days. Once the body adjusts, they’re kept on a daily maintenance dose - usually 650 mg twice a day.
The results? 85% of patients see better asthma control. Sinus surgery needs drop by 60%. Polyp regrowth slows from every 6 months to every 2-3 years. One patient on the Samter’s Society forum, NoseFree99, said their polyps went from recurring every six months to every three years after desensitization.
It’s not risk-free. About 42% of patients have reactions during the process. That’s why it’s only done in specialized centers with emergency equipment on hand. But for those who complete it, the quality of life improvement is massive. A 2022 survey found 68% of patients reported significant gains.
What About Biologics and New Drugs?
Biologics like dupilumab (Dupixent) are now being used for AERD. It’s a shot that blocks IL-4 and IL-13 - two key players in the Type 2 inflammation that drives polyps and asthma.
Studies show it reduces polyp size by 50-60% and improves breathing. But it’s expensive - $38,500 a year - and only 38% of AERD patients have insurance coverage. It’s also not a replacement for aspirin desensitization. Many specialists use both together.
New drugs are coming. In June 2023, the FDA gave breakthrough status to MN-001 (lodadustat), a leukotriene inhibitor. Phase 2 trials showed a 70% drop in polyp recurrence. If it gets approved, it could be a game-changer for those who can’t tolerate daily aspirin.
Where to Get Help
There are only about 35 specialized AERD centers in the U.S. Most are tied to academic hospitals. Community clinics rarely offer desensitization - only 12% of allergy practices do.
If you suspect you have AERD, start by asking your doctor for a referral to an allergist-immunologist who specializes in respiratory diseases. Don’t settle for general care. This condition needs experts.
Support groups like the Samter’s Society (samterssociety.org) offer free resources: 127 articles, 28 patient videos, and a community of over 2,300 people who’ve been through it. Their patient portal has a 4.5/5 rating for clarity and usefulness.
Specialized centers also offer 24/7 nurse hotlines. One patient told me they got a call back in under two hours when they panicked after a reaction. At a regular clinic? They waited three days.
What You Can Do Today
If you have asthma and nasal polyps, and you’ve ever had a reaction to ibuprofen, aspirin, or alcohol - don’t wait. Write down your symptoms: when they happened, what you took, how long it took to react.
Ask your doctor: Could this be AERD? If they say no or don’t know, ask for a referral to an AERD specialist. You don’t need to suffer for another decade.
Don’t avoid NSAIDs just because you’re scared. Avoidance doesn’t stop the disease. It just leaves you stuck with worsening symptoms and repeated surgeries.
Desensitization is hard. It takes time. But for most people, it’s the only way to take back control of their breathing, their sense of smell, and their life.
Why This Matters
AERD affects 1.2 million Americans. It costs the system $1.8 billion a year in surgeries, ER visits, and lost workdays. But the human cost is higher.
People lose their sense of smell. They can’t enjoy food. They can’t sleep because their nose is blocked. They miss work, cancel plans, and live in fear of a simple painkiller.
And it’s worse for Black and Hispanic patients - they wait 3.2 years longer for diagnosis. That’s not just a gap. It’s a failure of the system.
This isn’t rare. It’s underdiagnosed. And it’s treatable.

Casper MacIntyre
Hello, my name is Casper MacIntyre and I am an expert in the field of pharmaceuticals. I have dedicated my life to understanding the intricacies of medications and their impact on various diseases. Through extensive research and experience, I have gained a wealth of knowledge that I enjoy sharing with others. I am passionate about writing and educating the public on medication, diseases, and their treatments. My goal is to make a positive impact on the lives of others through my work in this ever-evolving industry.
14 Comments
-
Bret Freeman
December 26, 2025 AT 06:31Let me be clear-this isn’t just a medical condition, it’s a betrayal by the pharmaceutical industry. They push NSAIDs like candy while knowing full well how many people are walking time bombs. And then they charge $38,500 a year for dupilumab like it’s a luxury watch. This isn’t healthcare-it’s corporate extortion wrapped in a white coat.
And don’t get me started on how they call it 'desensitization' like it’s some kind of magic trick. You’re literally poisoning yourself on purpose, under supervision, just to get back to baseline. That’s not treatment-that’s survival theater. -
Austin LeBlanc
December 27, 2025 AT 02:39You people are missing the point. This isn’t about drugs or biologics-it’s about personal responsibility. If you’re going to drink wine and take Advil and then wonder why you can’t breathe, maybe stop doing both. It’s not rocket science. Why are we medicalizing poor lifestyle choices?
And why are we giving these people free passes? You don’t see people with diabetes getting subsidized insulin because they ate a whole cake. Why should AERD patients get biologics because they won’t avoid triggers? This is enabling. -
niharika hardikar
December 28, 2025 AT 01:03It is imperative to underscore that the pathophysiology of Aspirin-Exacerbated Respiratory Disease is not merely a pharmacological anomaly, but a profound dysregulation of the arachidonic acid cascade, leading to an overproduction of cysteinyl leukotrienes and a concomitant deficiency in cytoprotective prostaglandins.
Moreover, the clinical triad of asthma, nasal polyposis, and NSAID intolerance remains underrecognized in global medical practice, particularly in low-resource settings where diagnostic infrastructure is lacking. The disparity in diagnosis timelines between Caucasian and non-Caucasian populations is a glaring indicator of systemic inequity in respiratory immunology care. -
EMMANUEL EMEKAOGBOR
December 28, 2025 AT 11:30This is a very important topic, and I appreciate the depth of the explanation. In Nigeria, many people with asthma are not even aware that common painkillers could trigger such severe reactions. We need more awareness campaigns, especially in rural areas where people self-medicate with whatever is available.
Also, the alcohol connection is something I’ve seen in my community-people blame the wine, not the inflammation. Education is the first step. Thank you for highlighting the Samter’s Society. We should share this with our medical associations. -
Jillian Angus
December 29, 2025 AT 20:40Been living with this for 12 years. Never knew alcohol was part of it until last year. One glass of wine and I’m gasping. My ENT thought I was being dramatic. Turns out I wasn’t. Now I’m on daily aspirin and my polyps haven’t grown back in 18 months. It’s not perfect but it’s better.
Also the smell thing. You don’t realize how much you miss it until it’s gone. -
Spencer Garcia
December 30, 2025 AT 01:16Aspirin desensitization works. I’ve seen it. But it’s not for everyone. If you’re on blood thinners or have a history of GI bleeds, you’re out. Also, the process is brutal-3 days of escalating doses, constant monitoring. You’re not just sitting there. You’re fighting for every breath.
But if you can get through it? Worth it. 85% improvement? That’s not a stat-that’s your life back. -
Blow Job
December 30, 2025 AT 01:52I used to think I just had bad allergies until I had a full asthma attack after taking ibuprofen for a headache. I thought I was dying. Took me two years to find out it was AERD. No one asked about alcohol. No one. My doctor just said 'avoid NSAIDs' and moved on.
Desensitization saved me. I can now drink wine without panicking. I can sleep. I can smell coffee again. I didn’t know how much I’d lost until I got it back.
If you’re reading this and you have polyps + asthma + NSAID reaction-go get tested. Don’t wait. It’s not a phase. It’s your body screaming. -
Christine Détraz
January 1, 2026 AT 00:26I think the real tragedy is how many people get misdiagnosed as having 'chronic sinusitis' or 'allergic asthma' and just get treated symptomatically. No one looks at the bigger picture. It’s like fixing a leaky roof without noticing the foundation is crumbling.
Also, the alcohol thing is so under-discussed. I didn’t realize my wine nights were triggering my asthma until I kept a journal. Now I don’t drink. It’s not hard. It’s just… different. -
John Pearce CP
January 2, 2026 AT 18:16It’s no surprise that this condition is more prevalent in Western countries where NSAID consumption is rampant. We’ve normalized taking painkillers like candy. And now we’re surprised when the body rebels?
Meanwhile, in traditional medicine systems-Ayurveda, TCM-there’s a deep understanding of inflammation and its triggers. We don’t need biologics. We need to stop poisoning ourselves with synthetic drugs and listen to our bodies.
Also, why are we funding expensive pharmaceutical trials instead of promoting dietary anti-inflammatories? This is capitalism masquerading as medicine. -
Gray Dedoiko
January 4, 2026 AT 09:26My sister has AERD. She had 4 sinus surgeries in 5 years. Each time, they’d say 'it’s gone, you’re good.' Then two months later-back again. She cried when she finally got the diagnosis. Not because she was upset, but because she finally understood why she’d been suffering for so long.
Desensitization was terrifying for her. But now? She’s been on aspirin for 2 years. No polyps. No ER visits. She even had a glass of wine at her wedding. I cried too.
This isn’t just a medical issue. It’s a human one. -
Joe Jeter
January 4, 2026 AT 18:57Let me guess-next you’ll tell me that the government is hiding a cure because Big Pharma makes more money off biologics. Right. And I’m sure the FDA is just sitting around waiting for someone to say 'let’s make people dependent on $40k/year shots.'
Here’s the truth: AERD is rare. It’s not a pandemic. It’s not even common. But now it’s a trend on Reddit. People are diagnosing themselves because they read a blog. Stop the fearmongering. -
Sidra Khan
January 6, 2026 AT 10:29Okay but why is it called Samter’s Triad? Who was Samter? Was he a guy who got mad at aspirin and then wrote a paper? 🤔
Also, I just Googled 'aspirin and wine' and the first result says 'don’t mix.' So… why are we having this conversation? I thought we were past 'don’t mix meds and alcohol' in 2005.
Also, I’m pretty sure I have this. My nose gets stuffy after a margarita. 🍹 #AERD #IHaveItNow -
Lu Jelonek
January 7, 2026 AT 12:42The data on diagnostic delays is staggering. But what’s more troubling is the lack of standardized screening tools. No one has a simple algorithm for primary care: 'If patient has adult-onset asthma + nasal polyps + NSAID reaction → refer to AERD specialist.'
It’s all anecdotal. We need a clinical decision support tool built into EHRs. It’s not complicated. And it would save lives. And money. And dignity.













Write a comment
More Articles

Improve Your Health and Vitality with Phleum Pratense Dietary Supplements
In my latest blog post, I delve into the health benefits of Phleum Pratense dietary supplements. Also known as Timothy Grass, this supplement has been linked to improved overall vitality and health. It's rich in antioxidants and can help boost immunity and soothe respiratory issues. I've also explored the potential for this supplement to aid in digestion and manage allergies. I strongly recommend giving it a try if you're looking to enhance your health naturally.
Generic Drug Approval Standards: Safety, Quality, and Strength Requirements
Generic drugs must meet the same safety, strength, and quality standards as brand-name drugs under FDA oversight. Learn how bioequivalence, manufacturing controls, and strict testing ensure they work just as well.
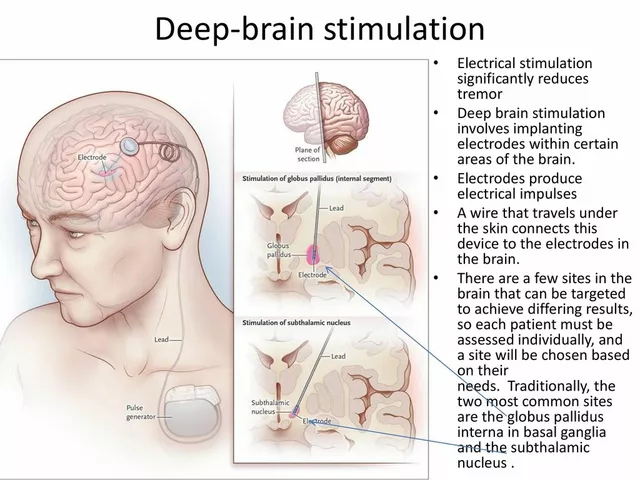
Deep Brain Stimulation for Tremor Management: A Comprehensive Guide
In my latest blog post, I've created a comprehensive guide on Deep Brain Stimulation (DBS) for tremor management. This innovative treatment has been proven to effectively reduce tremors in patients with Parkinson's disease and essential tremor. Through a surgical procedure, a device is implanted to send electrical signals to specific areas of the brain, offering relief to those struggling with involuntary shaking. I've included detailed information on the procedure, its benefits, and potential risks to help you better understand this life-changing treatment option. If you or a loved one are experiencing tremors, I highly recommend giving it a read to see if DBS could be the right solution for you.
Abby Polhill
December 25, 2025 AT 01:58So AERD isn't just an allergy-it's a metabolic cascade gone rogue. The COX-1 inhibition leading to leukotriene surges? That’s the core. And the fact that alcohol triggers it via the same pathway? Mind blown. This isn't 'can't have ibuprofen'-it's 'your entire Type 2 immune axis is dysregulated.'
Biologics like dupilumab make sense mechanistically-blocking IL-4/IL-13 hits the eosinophilic firestorm. But the cost? Criminal. Insurance denials are the real epidemic here.
And yes, the 7–10 year diagnostic delay? That’s systemic failure. Primary care docs still think 'asthma + polyps' = allergic rhinitis. They don't connect the dots to NSAID sensitivity. We need mandatory screening protocols for adult-onset asthma with polyps. Period.