Opioid-Induced Adrenal Insufficiency Risk Calculator
Why This Matters
Long-term opioids (>20 MME/day for >90 days) can suppress your body's stress response. Symptoms like fatigue and dizziness are often missed as early signs of adrenal insufficiency - a life-threatening condition.
Your Risk Level
Risk Factors
Symptoms
- Chronic fatigue
- Nausea and loss of appetite
- Dizziness when standing
- Muscle weakness
- Low mood
High Risk? Consult your physician immediately about adrenal function testing. Untreated OIAI can lead to fatal adrenal crisis.
Most people know opioids can cause constipation, drowsiness, or dependence. But few know that long-term opioid use can quietly shut down your body’s natural stress response - leading to a condition called opioid-induced adrenal insufficiency (OIAI). It’s rare. It’s subtle. And if missed, it can kill you.
What Exactly Is Opioid-Induced Adrenal Insufficiency?
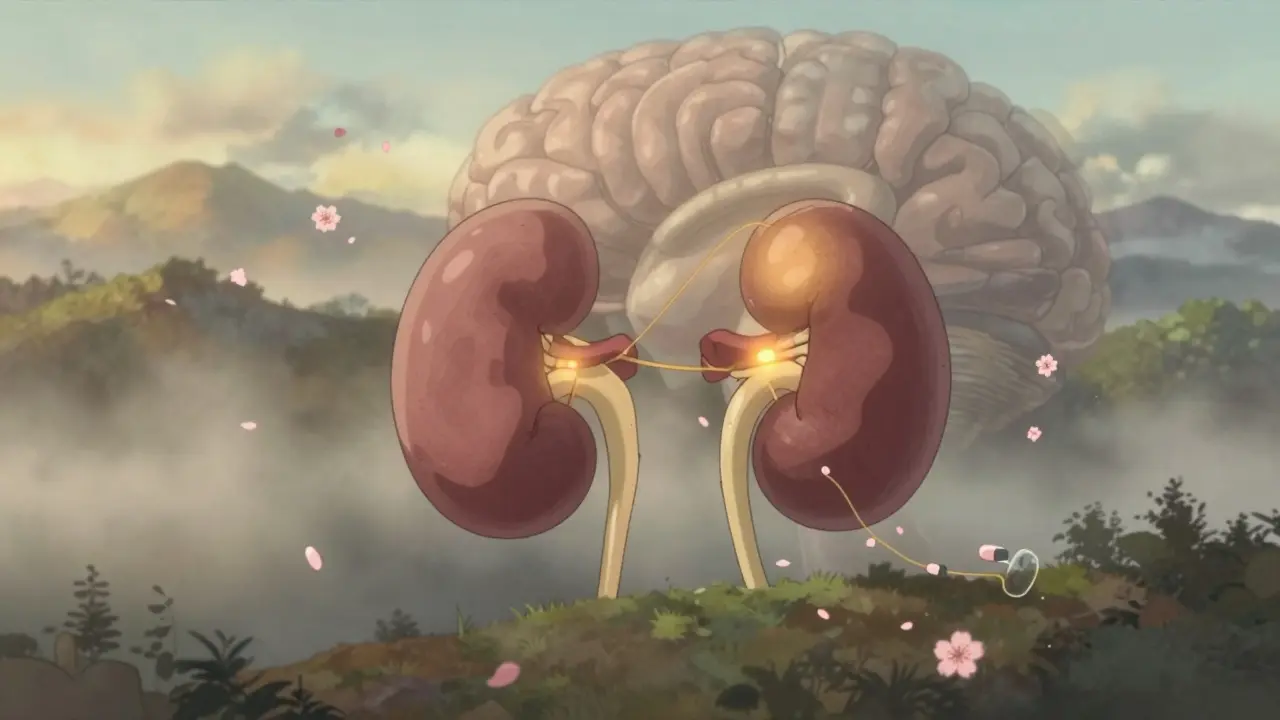
Your adrenal glands sit on top of your kidneys and produce cortisol - the hormone that keeps you alive during stress. Whether you’re in a car accident, fighting an infection, or having surgery, cortisol kicks in to raise your blood pressure, stabilize your blood sugar, and calm inflammation. Without it, your body can’t respond. That’s adrenal insufficiency. Opioids don’t damage your adrenals. Instead, they silence the chain of command: the hypothalamus and pituitary gland. These brain regions normally signal the adrenals to make cortisol. But opioids bind to receptors in the brain and block that signal. No signal = no cortisol. It’s like cutting the wire to a smoke alarm - the alarm still works, but no one’s telling it to go off. This isn’t new science. Studies from the 2010s already showed opioids suppress ACTH and cortisol. But for years, doctors didn’t connect the dots. Patients showed up tired, nauseous, low-blood-pressure, and were told they were just depressed or had the flu. Turns out, their bodies had run out of stress fuel.Who’s at Risk?
You don’t need to be on heroin. Prescription opioids are the main culprit. About 5% of adults in the U.S. are on chronic opioid therapy - that’s over 16 million people. And while not everyone develops adrenal insufficiency, the risk climbs sharply with dose and duration. If you’re taking more than 20 morphine milligram equivalents (MME) per day for longer than 90 days, your risk goes up. One study of 162 chronic opioid users found 5% had OIAI. Another, looking at patients on methadone or high-dose oxycodone, found 22.5% failed adrenal stimulation tests - compared to 0% in healthy controls. It doesn’t matter if you’re on oxycodone, hydrocodone, morphine, or methadone. All of them can do this. Even fentanyl patches. The key factors? Dose. Duration. And whether your body’s been under constant chemical suppression.What Are the Symptoms? (And Why They’re Easy to Miss)
OIAI doesn’t come with a flashing red light. Its symptoms look exactly like other things:- Chronic fatigue - "I’m just tired all the time"
- Nausea, loss of appetite - "I guess my pain is making me eat less"
- Dizziness when standing - "Must be low blood pressure from meds"
- Muscle weakness - "I’m getting older"
- Low mood - "I’m depressed from chronic pain"

How Is It Diagnosed?
There’s no blood test you can take at your GP’s office and get an instant answer. Diagnosis requires a stimulation test. The gold standard is the ACTH stimulation test. You get a shot of synthetic ACTH. Then, your cortisol levels are checked at 30 and 60 minutes. If your cortisol stays below 18 mcg/dL (or 500 nmol/L), your adrenals didn’t respond - meaning your brain isn’t telling them to work. Some newer research suggests even lower thresholds might be more accurate. A morning cortisol under 3 mcg/dL is a strong red flag, especially if you’re on high-dose opioids. The problem? Most doctors don’t order this test. Not unless they’re endocrinologists. And most pain clinics don’t screen for it. That’s why so many cases go undetected until it’s too late.Can It Be Reversed?
Yes. And that’s the good news. In one case, a 25-year-old man developed severe hypercalcemia after a critical illness. His doctors couldn’t figure out why - until they checked his cortisol. It was undetectable. He’d been on methadone for chronic pain. Once they stopped the methadone and gave him hydrocortisone, his cortisol returned to normal within weeks. His calcium levels stabilized. He recovered fully. This isn’t an outlier. Multiple case reports show the same pattern: stop or taper the opioid, give glucocorticoids during the transition, and the HPA axis slowly wakes up. It can take weeks to months. But the glands aren’t broken. They’re just asleep. Important note: you can’t just quit opioids cold turkey if you have OIAI. Your body needs steroid cover during withdrawal. Otherwise, you risk adrenal crisis. That’s why this needs to be managed by a doctor - not self-managed.What About Aldosterone? Do Opioids Affect Salt Balance?
Good question. Aldosterone is another hormone made by the adrenals. It controls sodium and potassium. Low aldosterone causes salt wasting, low blood pressure, and high potassium. Here’s the relief: opioids don’t suppress aldosterone. That’s because aldosterone is controlled by a different system - the renin-angiotensin system - not the HPA axis. So if you have low cortisol but normal sodium and potassium, that’s consistent with OIAI. If your potassium is high and sodium is low? Something else is going on.
Why Isn’t This More Widely Known?
Because it’s invisible until it’s deadly. The opioid epidemic has focused on overdoses, addiction, and withdrawal. But the slow, silent damage - like hormonal shutdown, low testosterone, and adrenal insufficiency - gets ignored. Studies show patients on long-term opioids report worse quality of life across physical, emotional, and social domains. Some of that is pain. Some of it is cortisol deficiency. Clinicians aren’t taught this in medical school. Guidelines don’t recommend routine screening. And when a patient says, "I’m always tired," the default answer is "depression" or "sleep apnea." Not "your adrenals stopped working because of your pain meds." But awareness is growing. Papers from 2020 to 2024 are calling for better screening. The American Medical Association’s Ed Hub now explicitly says: "Concern for OIAI should be raised in patients on chronic opioid therapy, particularly over 20 MME daily, with signs of adrenal insufficiency."What Should You Do If You’re on Long-Term Opioids?
If you’ve been on opioids for more than three months - especially at doses above 20 MME daily - and you feel constantly tired, dizzy, nauseous, or weak, ask your doctor one simple question: "Could this be opioid-induced adrenal insufficiency? Can we check my cortisol?" Don’t wait for a crisis. Don’t assume it’s "just pain." This is a treatable condition. And if caught early, it’s completely reversible. If your doctor doesn’t know what you’re talking about, bring them the research. Print out the 2024 review from Frontiers in Endocrinology. Point them to the ACTH stimulation test. Most will agree to order it if you’re persistent. And if you’re a clinician reading this? The next time someone on long-term opioids says they’re exhausted - don’t reach for the antidepressant. Reach for the cortisol test.Final Thought: It’s Not About Stopping Opioids - It’s About Safe Use
This isn’t a call to stop opioids. For many, they’re the only thing keeping pain manageable. But they’re not harmless. Every medication has trade-offs. Opioids help with pain. But they can also shut down your body’s emergency system. The goal isn’t fear. It’s awareness. If you’re on opioids long-term, your care team should be watching your hormones - not just your pain score. Because you can’t survive a crisis if your body has forgotten how to respond to one.
Casper MacIntyre
Hello, my name is Casper MacIntyre and I am an expert in the field of pharmaceuticals. I have dedicated my life to understanding the intricacies of medications and their impact on various diseases. Through extensive research and experience, I have gained a wealth of knowledge that I enjoy sharing with others. I am passionate about writing and educating the public on medication, diseases, and their treatments. My goal is to make a positive impact on the lives of others through my work in this ever-evolving industry.
11 Comments
-
Brady K.
January 2, 2026 AT 01:02Let’s cut through the noise: OIAI isn’t rare - it’s underdiagnosed because lazy clinicians default to ‘depression’ instead of running a basic ACTH test.
20 MME/day for 90+ days? That’s not ‘pain management,’ that’s endocrine sabotage. If you’re on chronic opioids and your energy’s been flatlining since Day 30 - stop blaming stress. Get your cortisol checked. Period.
And if your doc doesn’t know what ACTH is? Find a new one. Your adrenal glands aren’t optional. -
Robb Rice
January 2, 2026 AT 21:24Thank you for sharing this vital information. I had no idea that opioids could suppress the HPA axis in this way.
I’ve been on oxycodone for chronic back pain for over two years now, and I’ve always felt this low-grade fatigue - I thought it was just part of aging or the pain itself.
I’ll be scheduling an appointment with my doctor this week to ask about cortisol testing. I appreciate the clarity and the call to action.
It’s scary to think how many people are walking around with silent adrenal shutdown and no idea. -
Harriet Hollingsworth
January 4, 2026 AT 16:50This is why people shouldn’t be on opioids for ‘chronic pain’ in the first place. You’re just trading one problem for ten others. It’s not medicine - it’s chemical surrender.
My cousin died from an ‘adrenal crisis’ after being on hydrocodone for 5 years. They never tested her cortisol. She was just ‘tired’ and ‘depressed.’
Stop enabling this. Stop prescribing it. Stop pretending it’s safe.
There are better ways. You just don’t want to find them. -
Bennett Ryynanen
January 6, 2026 AT 13:48Bro. I was on 80 MME for 3 years after my surgery. I thought I was just ‘burnt out.’ Turned out my cortisol was 1.2. My doc laughed at me when I asked about it. Said I was ‘overthinking.’
Then I got pneumonia last winter and nearly died. They had to give me IV steroids in the ER. That’s when they finally checked. Turns out I had OIAI.
Now I’m off opioids and on hydrocortisone. I feel like a human again.
If you’re on long-term pain meds and you’re always dragging - don’t wait for a crisis. Ask. Now. Your life depends on it. -
Chandreson Chandreas
January 6, 2026 AT 20:54Wow this is wild 🤯
I’m on methadone for nerve pain and I’ve been feeling like a zombie for 2 years. My wife says I don’t react to anything anymore - not even when the dog barks.
Maybe this is why.
Going to print this out and show my doctor tomorrow 🙏
Thank you for sharing this 🌱 -
Darren Pearson
January 7, 2026 AT 23:59The clinical negligence surrounding opioid-induced adrenal insufficiency is a glaring indictment of contemporary medical education and institutional inertia. The fact that a condition with such profound mortality implications remains outside routine screening protocols speaks to a systemic failure in translational medicine.
One must question the epistemic authority of primary care physicians who lack familiarity with the hypothalamic-pituitary-adrenal axis modulation by exogenous opioids.
This is not a patient advocacy issue - it is a bioethical imperative. -
Stewart Smith
January 9, 2026 AT 23:24My mom’s on 40 MME daily. She’s been ‘depressed’ for years. No one ever checked her cortisol. She’s been told to ‘exercise more’ and ‘get more sleep.’
She almost didn’t make it through last year’s flu. They had to give her steroids in the ER. That’s when they finally figured it out.
I’m glad someone’s talking about this. I’m sending this to every doctor in her family. No one should go through that again. -
Retha Dungga
January 10, 2026 AT 19:43this is so real i had no idea opioids could do this like wow i thought it was just the pain making me tired but now i think my body just stopped working 😭 i need to ask my doctor
also i think we need to stop acting like pain meds are magic pills they’re not they’re like a loan with interest and the interest is your hormones -
Jenny Salmingo
January 12, 2026 AT 09:33My dad’s from South Africa and he’s been on opioids since his accident in 2018. He’s always been tired, but he never complained. He just smiled and said, ‘It’s just how it is.’
I’m going to send this to my aunt. She’s his caregiver. Maybe this will help her understand why he’s so quiet now.
Thank you for writing this. It’s not just medical - it’s human. -
Aaron Bales
January 14, 2026 AT 05:44If you’re on chronic opioids and feel constantly tired, dizzy, or nauseous - get a cortisol test. No excuses. No waiting. This is a simple, life-saving check.










Write a comment
More Articles
Sildamax vs Other Sildenafil Alternatives: Detailed Comparison
Compare Sildamax with other ED meds like Viagra, Cialis, Levitra, and supplements. See efficacy, cost, onset, duration, side effects, and get a decision guide.


Branden Temew
January 1, 2026 AT 21:42So let me get this straight - we’ve got a whole class of drugs that can turn your body’s emergency button into a mute switch, and the medical system’s still acting like it’s just a bad Yelp review? 😅
It’s like giving someone a chainsaw and then being shocked when they forget how to use a hammer.