
Delayed Medication Side Effect Risk Checker
Check Medication Safety Risk
When a patient suddenly develops a rash, joint pain, or even life‑threatening swelling months after starting a medication, the connection isn’t always obvious. Those are the classic moments when delayed medication side effects reveal themselves, often after a long stretch of uneventful use. This guide walks you through the why, how, and what‑to‑do so you can catch these late‑onset reactions before they turn serious.
What Counts as a Delayed Medication Side Effect?
In clinical terms, delayed medication side effects-or late‑onset adverse drug reactions (ADRs)-are harmful responses that surface hours, days, weeks, or even years after a drug is started. Unlike immediate reactions that appear within minutes, these ADRs hide behind a temporal gap, making the culprit hard to spot.
Delayed medication side effects are defined as unwanted drug‑induced events that manifest after 72 hours of exposure, often after a period of apparent safety. The World Health Organization estimates that about 5 % of all hospital admissions involve ADRs, with roughly 35 % of those being delayed reactions.
Common Types and Their Timing Patterns
Understanding the typical timeline helps triage symptoms. Here are the most frequently encountered delayed reactions:
- Type IV hypersensitivity (cell‑mediated) usually appears 48‑72 hours after exposure, but can stretch to 8 weeks.
- DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms) typically emerges 2‑8 weeks after the offending drug.
- Severe Cutaneous Adverse Reactions (SCARs) such as Stevens‑Johnson Syndrome (SJS) or Toxic Epidermal Necrolysis (TEN) often present 1‑3 weeks after drug initiation.
- Organ‑specific delayed effects-like tendon rupture from fluoroquinolones-may not appear until 3‑6 months post‑therapy.
- Metabolic or skeletal complications (e.g., osteoporosis from chronic corticosteroid use) can take years to become clinically evident.
Medication Classes Most Often Linked to Delayed Reactions
Not every drug carries the same delayed‑reaction risk. The following five groups dominate the landscape:
| Drug Class | Typical Delayed Reaction | Usual Onset | Potential Severity |
|---|---|---|---|
| ACE inhibitors | Angioedema | Months‑to‑years | Life‑threatening airway obstruction |
| Fluoroquinolones | Tendon rupture, peripheral neuropathy | 3‑6 months post‑treatment | Permanent disability |
| Proton pump inhibitors (PPIs) | Vitamin B12 & magnesium deficiency, chronic kidney disease | 2‑4 years of continuous use | Fracture risk, neurologic symptoms |
| Corticosteroids | Osteoporosis, cataracts, diabetes | Years of therapy | Increased fracture & infection risk |
| Antiepileptic drugs | DRESS, Stevens‑Johnson Syndrome | 2‑6 weeks | 5‑50 % mortality depending on phenotype |

Red Flags: Symptoms That Should Prompt a Drug Review
Delayed reactions can affect almost any organ system. Keep an eye out for these patterns:
- Cutaneous clues: New rash, pustules, or severe blistering that doesn’t fit a typical allergy timeline.
- Respiratory warning: Sudden tongue or airway swelling, especially in patients on ACE inhibitors.
- Musculoskeletal signs: Unexplained tendon pain or rupture weeks after finishing a fluoroquinolone course.
- Metabolic shifts: Gradual bone loss, high blood sugar, or cataract formation in long‑term steroid users.
- Systemic involvement: Fever, eosinophilia, and organ dysfunction (liver, kidney) appearing weeks after starting an antiepileptic.
When any of these appear without a clear alternative cause, ask yourself: "Could a medication started months ago be the trigger?"
How to Diagnose a Delayed Reaction
Because the timing is vague, a systematic approach is key.
- Comprehensive medication list: Include over‑the‑counter drugs, supplements, and herbal products.
- Timeline reconstruction: Chart when each drug was started, any dose changes, and when symptoms first appeared.
- Laboratory testing: CBC with differential (look for eosinophilia), liver/kidney panels, and serum drug levels if applicable.
- Specialized tests:
- Lymphocyte transformation test (85‑90 % sensitivity for Type IV hypersensitivity).
- Skin patch testing (70‑80 % accuracy when done 4‑6 weeks after the acute event).
- Genetic screening: HLA‑B*57:01 for abacavir, HLA‑B*15:02 for carbamazepine‑induced SJS/TEN. These are becoming standard in many hospitals.
Collaboration with an allergist or clinical pharmacologist often speeds up identification.
Management Strategies Once a Delayed ADR Is Confirmed
Stopping the offending drug is the first, non‑negotiable step. Afterward, treatment depends on severity:
- Mild cutaneous reactions: Topical steroids, antihistamines, and close monitoring.
- Severe SCARs (SJS/TEN, DRESS): Hospital admission, systemic corticosteroids or IVIG, supportive care, and early ophthalmology consult.
- Musculoskeletal injuries (tendon rupture): Orthopedic evaluation, surgical repair, and rehabilitation.
- Metabolic complications: Bone density testing, vitamin supplementation, endocrinology referral.
Never re‑challenge a drug that caused a serious delayed reaction. For milder cases, cross‑reactivity must be assessed before choosing an alternative.

Prevention: Reducing the Risk of Late‑Onset Reactions
Prevention is a mix of vigilant prescribing and patient education.
- Risk assessment before prescribing: Review age, comorbidities, and known genetic markers.
- Educate patients about timelines: Explain that some side effects can appear months later and encourage them to report new symptoms.
- Regular medication reviews: At each clinic visit, reconcile the drug list and consider deprescribing when long‑term risk outweighs benefit.
- Use electronic alerts: Many EHR systems now flag high‑risk drug‑patient combos (e.g., fluoroquinolones in older adults).
- Consider prophylactic supplementation: For long‑term PPIs, check magnesium and B12 levels annually.
These steps have already cut delayed ADR hospitalizations by up to 12 % in health systems that adopted systematic review protocols.
Key Takeaways
- Delayed medication side effects can appear from days to years after drug start, often hiding behind normal use.
- Common culprits include ACE inhibitors, fluoroquinolones, PPIs, corticosteroids, and antiepileptic drugs.
- Watch for skin eruptions, unexplained swelling, tendon pain, metabolic shifts, or multi‑organ involvement.
- Diagnose by mapping drug timelines, using lab tests, and, when needed, specialized allergy testing or genetic screening.
- Prompt drug cessation, appropriate supportive care, and thorough patient education are the cornerstones of management and prevention.
Frequently Asked Questions
How long after starting a medication can a delayed side effect appear?
It varies widely-some reactions show up within 48 hours, while others, like osteoporosis from steroids, may take years. Most serious delayed hypersensitivity reactions appear between 2 weeks and 8 weeks.
Can genetic testing prevent delayed reactions?
Yes, for certain drugs. HLA‑B*57:01 testing prevents abacavir hypersensitivity, and HLA‑B*15:02 screening reduces carbamazepine‑related SJS/TEN. More panels are expected to become routine by 2025.
What should I do if I suspect a delayed reaction?
Stop the suspect drug immediately, contact your healthcare provider, and note the exact timing of symptom onset. Bring a complete medication list to your appointment.
Are over‑the‑counter supplements also a risk?
Absolutely. Supplements like calcium or herbal extracts can interact with prescription drugs and trigger delayed hypersensitivity, especially in people with prior reactions.
How common are delayed adverse reactions?
The FDA’s FAERS database recorded 2.3 million adverse events in 2022, with about 35 % classified as delayed. That translates to millions of patients worldwide each year.
Can lifestyle changes lower my risk?
Staying active, maintaining a healthy weight, and avoiding smoking reduce overall inflammation, which can lessen the severity of hypersensitivity reactions. Regular labs also catch early metabolic side effects.
Delayed medication side effects are a hidden but manageable part of modern pharmacotherapy. By staying alert to timing, symptoms, and risk factors, both patients and clinicians can intervene early, avoid serious complications, and keep treatment safe and effective.

Casper MacIntyre
Hello, my name is Casper MacIntyre and I am an expert in the field of pharmaceuticals. I have dedicated my life to understanding the intricacies of medications and their impact on various diseases. Through extensive research and experience, I have gained a wealth of knowledge that I enjoy sharing with others. I am passionate about writing and educating the public on medication, diseases, and their treatments. My goal is to make a positive impact on the lives of others through my work in this ever-evolving industry.
13 Comments
-
Benjamin Sequeira benavente
October 25, 2025 AT 19:16Alright folks, let’s get moving on this! 🚀 Keep a notebook on every med you start and note the date – it’s a game‑changer.
If something weird pops up months later, you’ll have the timeline ready to show your doc.
Don’t wait for the doctor to ask – be the one asking the hard questions.
Remember, early detection can save you from a nasty hospitalization.
Stay on top of it, stay healthy! -
Shannon Stoneburgh
October 26, 2025 AT 16:29Another endless list of drug side‑effects that nobody reads until it’s too late.
Patients are left scrambling for explanations after months of “perfect” therapy.
This guide just repeats the obvious without any new insight.
Save us the fluff. -
Nathan Comstock
October 27, 2025 AT 14:43Only in the United States do we have the resources to actually investigate these delayed reactions.
Our FDA has the toughest post‑marketing surveillance, unlike those other countries that just sweep problems under the rug.
Patriotic doctors should be proud of how we tackle ADRs head‑on.
Keep supporting the system that keeps us safe. -
Terell Moore
October 28, 2025 AT 12:56Ah, the ever‑expanding lexicon of delayed adverse drug reactions – a true masterpiece of modern pharmacology’s self‑congratulation.
One might wonder whether the exhaustive tables and timelines are intended to educate clinicians or merely to inflate the page count of yet another “guideline” document.
Consider the irony that while we laud evidence‑based practice, we often cling to anecdotal case reports that lack rigorous validation.
The reliance on lymphocyte transformation tests, with their touted 85‑90 % sensitivity, reeks of a false sense of security, especially when the gold standard remains a clinical judgment that is, frankly, all too subjective.
Moreover, the emphasis on genetic screening for HLA‑B*57:01 or HLA‑B*15:02, though commendable, glosses over the socioeconomic barriers that render such testing inaccessible to the majority of patients who might benefit most.
And let us not forget the charmingly obtuse phrase “life‑threatening airway obstruction” that is tossed around when discussing ACE‑inhibitor angioedema – a reminder that fear mongering is still a preferred pedagogical tool.
One could argue that the proliferation of electronic alerts in EHRs, designed to flag high‑risk combinations, merely adds to alarm fatigue, causing clinicians to ignore the very warnings meant to protect them.
In the same breath, the guide’s suggestion to supplement long‑term PPI users with magnesium and B12 is solid, yet it fails to address the root cause: the over‑prescription of PPIs in the first place.
Indeed, the cascade of downstream interventions – from orthopedic repair of fluoroquinolone‑induced tendon ruptures to endocrinology referrals for steroid‑induced osteoporosis – paints a picture of a healthcare system more adept at treating complications than preventing them.
While the article applauds “regular medication reviews,” it provides no concrete framework for how busy clinicians can practically execute such reviews amidst mounting administrative burdens.
Is the solution truly increased vigilance, or should we be questioning the very necessity of these high‑risk medications in the first place?
In summary, the guide is a commendable compendium of known facts, yet it stops short of challenging the paradigms that generate these delayed reactions.
Perhaps the next edition will dare to ask whether we need fewer drugs, not just better detection methods.
Until then, we continue to navigate a labyrinth of side‑effects, armed with tables, tests, and a healthy dose of skepticism. -
Amber Lintner
October 29, 2025 AT 11:09Wow, look at all the drama over a rash that shows up a month later.
Honestly, people love to turn every little symptom into a medical crisis.
Maybe it’s just a coincidence, not a grand conspiracy of delayed side‑effects.
Let’s not blow this out of proportion. -
Lennox Anoff
October 30, 2025 AT 09:23It is morally incumbent upon clinicians to safeguard patients from hidden pharmaceutical hazards.
When a drug can silently sabotage health months after prescription, silence is tantamount to complicity.
We must demand transparency and rigorous post‑marketing surveillance.
Only then can we align medical practice with the ethical duty to do no harm. -
Olivia Harrison
October 31, 2025 AT 07:36Hey there! Just wanted to add a quick friendly recap.
Keep an eye on any new skin changes, swelling, or joint pain after you start a new medication, even if it’s been weeks or months.
Write down when you started each drug and bring that list to your next appointment.
If something feels off, call your provider sooner rather than later.
Staying proactive really makes a difference! -
Bianca Larasati
November 1, 2025 AT 05:49Let’s keep the energy up, everyone! 🚀 Monitoring meds isn’t boring – it’s the key to catching those sneaky delayed reactions before they turn into big problems.
Set a reminder on your phone, make a simple chart, and share it with a friend who can help you stay accountable.
We’ve got this! -
Corrine Johnson
November 2, 2025 AT 04:03Fascinating, really!; the sheer volume of data on delayed adverse drug reactions-statistics, timelines, genetic markers--is staggering!!!
One cannot help but marvel at the complexity; however, the practical application remains elusive; clinicians are left wading through layers of nuance!!!
Thus, a call for clarity, brevity, and actionable steps is paramount!!! -
Jennifer Stubbs
November 3, 2025 AT 02:16From a balanced perspective, the guide highlights key red flags while also acknowledging that not every symptom is drug‑related.
It’s prudent to consider alternative diagnoses, but maintaining a high index of suspicion for delayed ADRs can prevent serious outcomes.
Overall, a useful resource for clinicians. -
Abhinav B.
November 4, 2025 AT 00:29Yo bro, thsi is reallly important!!!
Dont just polp up a meds list and forget it – keep it on your phone and check it evry month.
Pharma cant do hidden tings if we stay awar e. -
Ken Dany Poquiz Bocanegra
November 4, 2025 AT 22:43While the extensive analysis is thorough, the pragmatic takeaway remains simple: track medication timelines, stay alert for the listed red flags, and act quickly when symptoms arise.












Write a comment
More Articles

Low Density Living and Lower Crime Rates: Why Space Matters
Explore how low density residential layouts influence crime rates, the role of social cohesion, design strategies, and policy tools that make neighborhoods safer.
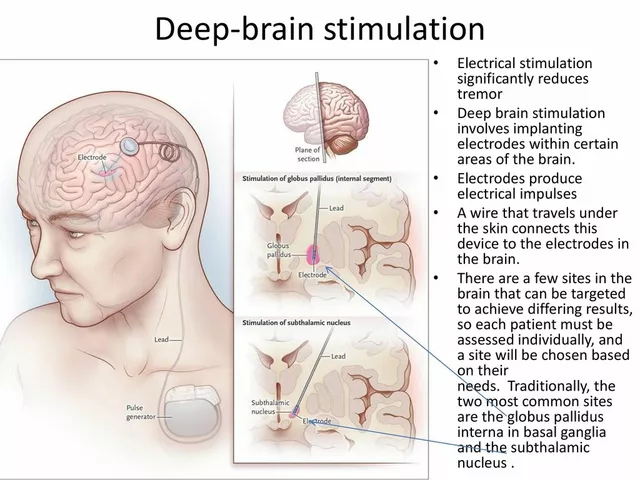
Deep Brain Stimulation for Tremor Management: A Comprehensive Guide
In my latest blog post, I've created a comprehensive guide on Deep Brain Stimulation (DBS) for tremor management. This innovative treatment has been proven to effectively reduce tremors in patients with Parkinson's disease and essential tremor. Through a surgical procedure, a device is implanted to send electrical signals to specific areas of the brain, offering relief to those struggling with involuntary shaking. I've included detailed information on the procedure, its benefits, and potential risks to help you better understand this life-changing treatment option. If you or a loved one are experiencing tremors, I highly recommend giving it a read to see if DBS could be the right solution for you.
krishna chegireddy
October 24, 2025 AT 21:03They don’t want you to know that Big Pharma has been hiding delayed reactions for decades.
Every new pill comes with a silent clause that the worst side‑effects might show up months later.
It’s not a coincidence that the most serious cases come after the drug is assumed safe.
Think about the millions of prescriptions written without a single follow‑up question about future safety.
Trust is a luxury in an industry that profits from secrecy.
When you see a rash weeks after stopping antibiotics, ask yourself who benefits from your ignorance.
Look beyond the label, the fine print is where the truth hides.
Only a vigilant patient can catch the tricks they try to conceal.
Stay skeptical, stay alive.