When older adults take medications, their kidneys don’t work the same way they did when they were younger. That’s not just a vague concern-it’s a real risk. About 30% of the most common drugs prescribed to seniors are cleared by the kidneys. If those kidneys aren’t working well, and dosing isn’t adjusted, toxicity can happen. A simple blood pressure pill, an antibiotic, or even a blood thinner can become dangerous. This isn’t about rare side effects. It’s about routine care that’s often done wrong.
Why Kidney Function Changes with Age
Your kidneys naturally slow down as you get older. By age 70, the average person loses about 40% of their kidney filtering capacity compared to when they were in their 20s. That’s not disease. That’s aging. The number of working filtering units (nephrons) drops. Blood flow to the kidneys decreases. Muscle mass shrinks, which changes how creatinine-a key marker doctors use-is made and cleared.
This means a “normal” creatinine level in a 75-year-old might actually mean their kidneys are barely working. If you rely on that number alone, you’ll underestimate how poorly their kidneys are functioning. And that’s when dosing errors happen.
The Equations Doctors Use (and Why They’re Not All Equal)
Doctors don’t measure kidney function directly. They estimate it using equations. But not all equations are made for seniors. The most common ones are:
- Cockcroft-Gault (CG) - Developed in 1976. Uses age, weight, sex, and serum creatinine.
- MDRD - Created in 1999. Designed for people with chronic kidney disease, not healthy seniors.
- CKD-EPI - Introduced in 2009. Now the most common in electronic health records.
- BIS1 and FAS - Newer equations built specifically for older adults.
Here’s the problem: CKD-EPI and MDRD were designed for younger, sicker patients. In people over 75-especially those who are thin, frail, or have low muscle mass-these equations often overestimate kidney function by 15 to 30%. That’s not a small mistake. It’s the difference between a safe dose and a toxic one.
For example, a study of 1,200 seniors found that using the standard Cockcroft-Gault formula with actual body weight led to dosing errors in 32% of cases. But when they switched to using ideal body weight in the same formula, errors dropped to 7%. That’s a 25-point improvement just by changing one input.
Why BIS1 and FAS Are Better for Seniors
BIS1 (Berlin Initiative Study 1) and FAS (Full Age Spectrum) were developed because researchers realized older adults needed their own equations. These take into account age, sex, serum creatinine, and also factors like body composition and frailty.
Studies show BIS1 is more accurate than CKD-EPI in people over 80. In one trial, BIS1 correctly classified kidney function in 95% of cases, while CKD-EPI got it right in only 78%. That might sound technical, but here’s what it means in practice:
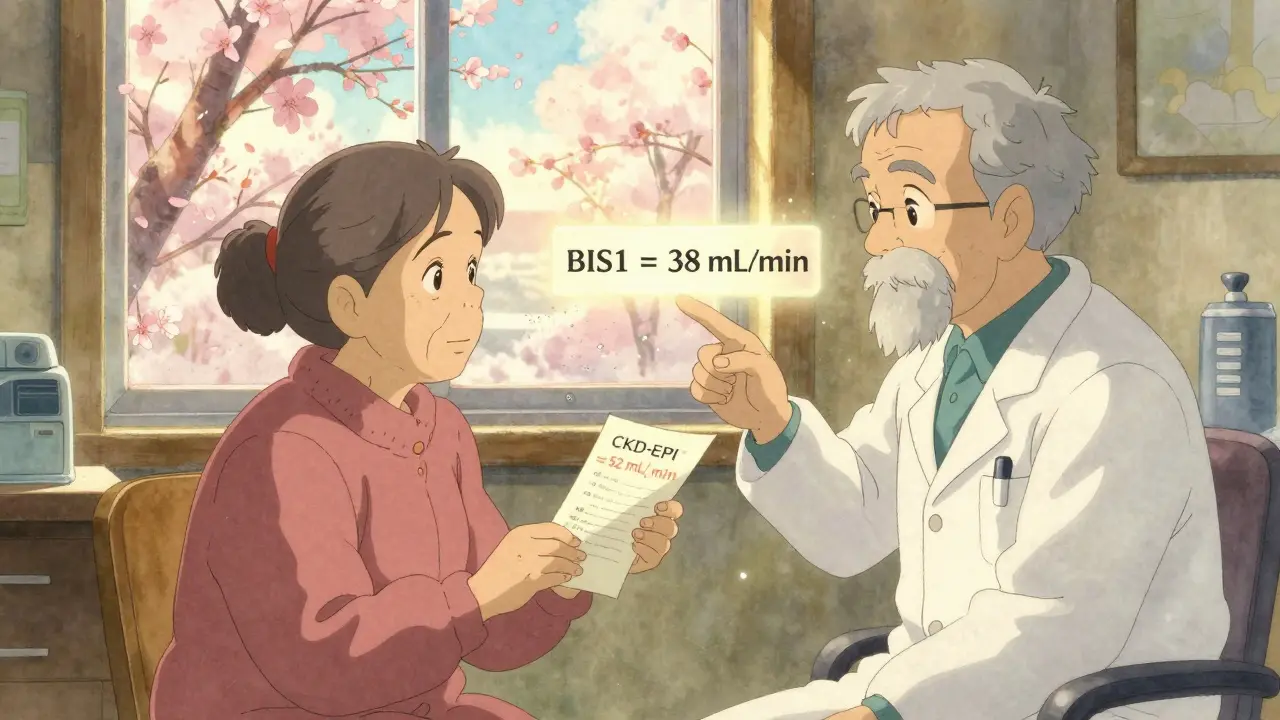
- A 82-year-old woman with low muscle mass might have an eGFR of 52 mL/min using CKD-EPI.
- Using BIS1, the same person’s eGFR might be 38 mL/min.
- That changes her dosing for drugs like dabigatran or vancomycin-drugs where even a 20% overdose can cause serious harm.
Dr. Sophie Dupont’s team at the University of Michigan found that switching from CKD-EPI to BIS1 in patients over 80 reduced medication-related hospitalizations by 18%. That’s not just a number-it’s real people avoiding ER visits, falls, bleeding, or kidney failure.
When Creatinine Isn’t Enough
There’s another tool: cystatin C. Unlike creatinine, it’s not affected by muscle mass. That makes it much more reliable in seniors who are thin, bedridden, or malnourished.
But cystatin C tests cost $50-$75 more than a regular creatinine test. So it’s not done routinely. But here’s when it should be:
- Your creatinine looks normal, but you’re frail, losing weight, or have no muscle.
- Your eGFR from CKD-EPI says you’re in Stage 2 (mild decline), but you’re on a drug that needs strict dosing.
- You’ve had a recent fall or infection, and your creatinine suddenly dropped.
When cystatin C is added to creatinine, the accuracy improves. New equations like CKD2024 combine both markers and show 15% better accuracy in people over 80. This isn’t science fiction-it’s available now.
What Actually Happens in Clinics
Most electronic health records default to CKD-EPI. That’s convenient. But it’s not safe for seniors.
A 2023 survey found that 65% of primary care doctors feel unsure about which equation to use. Nearly half just go with whatever the computer picks. That’s dangerous.
Pharmacists in nursing homes report overriding EHR defaults at least once a week. One pharmacist wrote: “I’ve seen more harm from using the wrong equation than from any single drug’s side effect.”
Some hospitals are catching on. Epic Systems now automatically uses BIS1 for patients over 75. But most community clinics still rely on outdated defaults.
How to Get It Right
If you’re a senior, or caring for one, here’s how to make sure kidney function is handled correctly:
- Ask which equation was used-not just “Is my kidney function normal?” Ask: “Was it CKD-EPI, MDRD, or BIS1?”
- Check your weight and muscle status-If you’ve lost weight, are frail, or have little muscle, BIS1 or cystatin C may be needed.
- Review all medications-Drugs like warfarin, digoxin, gabapentin, and many antibiotics need adjustment. Ask your pharmacist to check each one.
- Request a cystatin C test-If your creatinine is normal but you’re at risk, this test is worth the cost.
- Use updated tools-The National Kidney Foundation’s eGFR calculator (updated 2023) and the American Geriatrics Society’s 2024 toolkit let you plug in numbers and compare equations.
The Bigger Picture
This isn’t just about dosing. It’s about how medicine treats aging. We assume “normal” lab values apply to everyone. But a 70-year-old with 40% kidney function isn’t “normal.” They’re just old.
Regulators are starting to notice. The FDA now requires drug makers to provide dosing guidance using multiple equations for older adults. Medicare is penalizing hospitals for medication errors in seniors. These are real consequences.
But change is slow. The best defense is knowledge. If you’re taking more than three medications, ask your doctor: “Which kidney function equation was used to calculate my dose? Is it the right one for me?”
There’s no magic test. No single equation works for everyone. But the right choice can mean the difference between staying healthy and ending up in the hospital.
What’s the best equation for estimating kidney function in seniors over 75?
For seniors over 75, especially those who are frail, thin, or have low muscle mass, the BIS1 or FAS equations are more accurate than CKD-EPI or MDRD. Studies show BIS1 reduces dosing errors by up to 25% in this group. While CKD-EPI is still the default in most electronic health records, geriatric specialists recommend BIS1 for patients over 75 because it accounts for age-related changes in body composition that older equations ignore.
Why is creatinine not reliable for older adults?
Creatinine is a waste product from muscle breakdown. As people age, they lose muscle mass-even if they don’t lose weight. This means less creatinine is produced, so blood levels can look normal even when kidney function is low. As a result, creatinine-based equations like CKD-EPI often overestimate kidney function in seniors by 15-30%, leading to unsafe medication doses.
Should I get a cystatin C test?
Yes, if you’re over 70, have low muscle mass, are losing weight, or are on medications that require precise dosing (like blood thinners or antibiotics). Cystatin C isn’t affected by muscle loss, so it gives a clearer picture of kidney function. It costs $50-$75 more than a creatinine test, but it can prevent dangerous overdoses. Ask your doctor if it’s right for you.
Do all pharmacies and doctors use the same method?
No. Most electronic health records automatically use CKD-EPI, even for seniors. But many pharmacists and geriatric specialists override this. A 2023 survey found 63% of pharmacists in senior care settings manually change the equation at least once a week to match the patient’s real condition. Academic centers are more likely to use BIS1, but community clinics often stick with defaults-putting patients at risk.
Can I calculate my own kidney function?
Yes, using free, updated tools. The National Kidney Foundation’s online eGFR calculator (updated November 2023) lets you enter your age, sex, race, serum creatinine, and weight, then compares results from multiple equations. You can also use the American Geriatrics Society’s 2024 clinical toolkit. Bring the results to your doctor to discuss whether your current dosing is appropriate.
Next Steps for Seniors and Caregivers
If you’re managing medications for yourself or someone else:
- Keep a list of all medications and dosages.
- Ask for the latest creatinine and eGFR results at every visit.
- Request BIS1 or cystatin C if there’s any doubt about kidney function.
- Don’t assume “normal” lab results mean safe dosing.
- Use the National Kidney Foundation’s calculator to compare results before your next appointment.
Medication safety in older adults isn’t about doing more tests. It’s about doing the right test. And that starts with asking the right question.

Casper MacIntyre
Hello, my name is Casper MacIntyre and I am an expert in the field of pharmaceuticals. I have dedicated my life to understanding the intricacies of medications and their impact on various diseases. Through extensive research and experience, I have gained a wealth of knowledge that I enjoy sharing with others. I am passionate about writing and educating the public on medication, diseases, and their treatments. My goal is to make a positive impact on the lives of others through my work in this ever-evolving industry.
14 Comments
-
Carrie Schluckbier
February 15, 2026 AT 22:55Let me guess-this was written by Big Pharma. BIS1? FAS? Those aren't 'new equations'-they're Trojan horses. The real goal is to make seniors dependent on more expensive tests so insurers can jack up premiums. Cystatin C costs $75? That's a profit center. Meanwhile, real kidney function is measured by urine output and clinical signs-not some algorithm that needs a PhD to decode.
-
Liam Earney
February 17, 2026 AT 09:43You know, I’ve been thinking about this for a while now… and it’s not just about equations… it’s about how we’ve medicalized aging… we treat old age like a disease to be corrected… rather than accepting it as a natural state… I remember my grandmother… she was 84… her creatinine was ‘normal’… but she couldn’t climb stairs… and they gave her a statin… and then she fell… and then… well… you know how this story ends…
-
guy greenfeld
February 18, 2026 AT 01:58The real issue here isn't the equations-it's the epistemological crisis in modern medicine. We've outsourced clinical judgment to algorithms because we're terrified of uncertainty. But the human body isn't a spreadsheet. A 75-year-old woman with 38 mL/min isn't 'chronic kidney disease'-she's just old. And we've forgotten how to care for old people without turning them into data points. This isn't science. It's scientism.
-
Sam Pearlman
February 18, 2026 AT 15:50I'm a pharmacist and I override EHR defaults every single day. I had a guy on warfarin with a CKD-EPI of 55-BIS1 said 39. I called his doc, they laughed. Two weeks later, he was in the ER with a GI bleed. Don't let the system fool you. You have to be your own advocate. And yes, it's exhausting-but worth it.
-
Jonathan Ruth
February 19, 2026 AT 08:54CKD EPI is fine. Stop overcomplicating. If your grandma is on meds and her creatinine is normal then she's fine. The real problem is people taking 12 pills a day and expecting miracles. Stop looking for hidden dangers in every lab result. Your kidneys don't need a PhD to function.
-
Philip Blankenship
February 20, 2026 AT 20:47I read this whole thing and just nodded along. My mom's 81, frail, weighs 98 lbs, and her creatinine was 'normal' for years. We finally got cystatin C done last month-eGFR dropped from 54 to 37. Her doc didn't even know BIS1 existed. Now she's on a lower dose of her heart med and actually has more energy. It's wild how something so simple gets overlooked. Just ask. Always ask.
-
Kancharla Pavan
February 22, 2026 AT 17:14This is why Western medicine is failing. We treat the elderly like broken machines instead of human beings with dignity. You don't need equations-you need respect. If a person is frail, you give them less medicine, not more. The fact that we need a 2000-word article to explain that shows how far we've fallen. In India, we don't calculate eGFR-we observe. Does the person walk? Eat? Sleep? That's what matters.
-
Dennis Santarinala
February 24, 2026 AT 15:08This is one of the most important posts I've read this year. Seriously. I'm sharing this with my entire family. My dad's 76, and we're going to ask for BIS1 at his next appointment. I never realized how much risk he was in just because a computer defaulted to the wrong formula. Thank you for writing this. It's not just medical-it's personal.
-
John Haberstroh
February 25, 2026 AT 22:34I love how the article calls out the difference between 'normal' and 'adequate.' A 70-year-old with 'normal' creatinine isn't normal-they're just old. And we treat aging like a glitch in the system instead of the natural state it is. It's like trying to fit a 1987 Toyota into a 2024 repair manual. The parts are the same, but the context? Totally different. We need more people thinking like this.
-
Logan Hawker
February 26, 2026 AT 21:16The BIS1 equation? Sounds like another overengineered academic vanity project. Real clinicians don't need this. They use clinical judgment. Also, cystatin C is overpriced junk. It's not more accurate-it's just another way to monetize geriatric care. And why are we still using body weight? In 2024, we should be using DEXA scans. But no, let's keep throwing money at outdated metrics.
-
James Lloyd
February 27, 2026 AT 21:49As a geriatric pharmacist, I've been advocating for BIS1 and cystatin C for over a decade. The data is solid. CKD-EPI overestimates eGFR by 20-30% in frail seniors. That’s not a nuance-it’s a safety hazard. I’ve reviewed over 500 charts in nursing homes. In 83% of cases, the default eGFR was dangerously high. The fix? Simple: change the EHR defaults. But bureaucracy moves slower than molasses in January.
-
Steph Carr
March 1, 2026 AT 02:31I live in a country where the average person takes 7 meds a day and no one checks their kidneys. I just asked my 72-year-old neighbor if she knew which equation they used for her dose. She looked at me like I asked if she believed in aliens. That’s the real crisis-not the algorithm. It’s the silence. No one asks. No one knows. And that’s terrifying.
-
Prateek Nalwaya
March 2, 2026 AT 19:37I'm from India and we don't have fancy equations here. We just watch. Does the person urinate? Do they feel weak? Do they vomit after pills? If yes-cut the dose. Simple. No lab. No calculator. Just observation. Maybe we're not 'scientific'-but we're not killing people with algorithms either. Sometimes, the oldest way is the safest.













Write a comment
More Articles
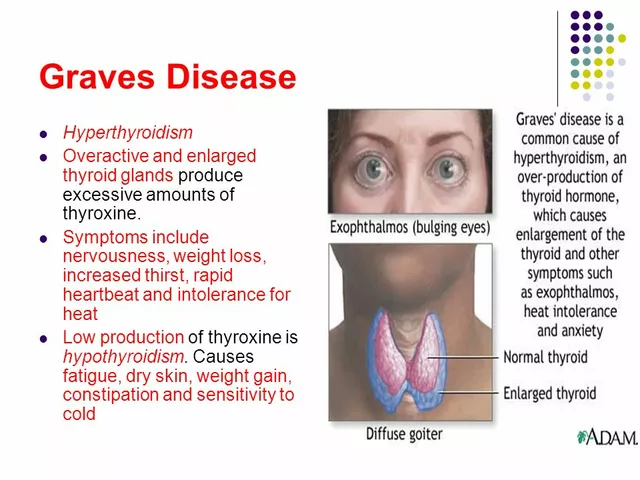
Diagnosing Graves' Disease: Signs, Symptoms, and Tests
I recently learned about Graves' disease, an autoimmune disorder that affects the thyroid gland. The common signs and symptoms include anxiety, weight loss, and a rapid heartbeat. It's important to be aware that some people might experience eye issues like bulging or discomfort. To diagnose this condition, doctors usually perform blood tests to measure thyroid hormone levels, and sometimes they might use imaging tests like ultrasounds. If you suspect you have Graves' disease, it's essential to consult with a healthcare professional to get a proper diagnosis and treatment plan.
180-Day Exclusivity: How Patent Law Shapes Generic Drug Market Entry
Explore how 180-day exclusivity under the Hatch-Waxman Act incentivizes generic drug companies to challenge patents and impact market pricing.

Improve Your Health and Vitality with Phleum Pratense Dietary Supplements
In my latest blog post, I delve into the health benefits of Phleum Pratense dietary supplements. Also known as Timothy Grass, this supplement has been linked to improved overall vitality and health. It's rich in antioxidants and can help boost immunity and soothe respiratory issues. I've also explored the potential for this supplement to aid in digestion and manage allergies. I strongly recommend giving it a try if you're looking to enhance your health naturally.
Tony Shuman
February 15, 2026 AT 20:45This is why America's healthcare system is broken. They use algorithms designed for 30-year-olds on 80-year-olds and call it 'evidence-based.' Meanwhile, real doctors who actually talk to patients are ignored. I've seen grandmas on blood thinners almost die because some EHR defaulted to CKD-EPI. No wonder people don't trust medicine anymore.